
For many clinicians, AI sounds promising until EHR (Electronic Health Records) integration enters the conversation. What begins as an interest in saving time often turns into a concern about long implementation cycles, vendor coordination, interface costs, and workflow disruption. For practices already stretched thin, the idea of months-long integration is often enough to stop adoption entirely.
But AI adoption doesn’t have to start with full EHR integration. In fact, for many practices, the most practical path forward is read-only EHR adoption, a lower-risk, faster way to introduce EHR-integrated AI documentation without operational headaches.
What is the Reality of Time Spent on EHR?
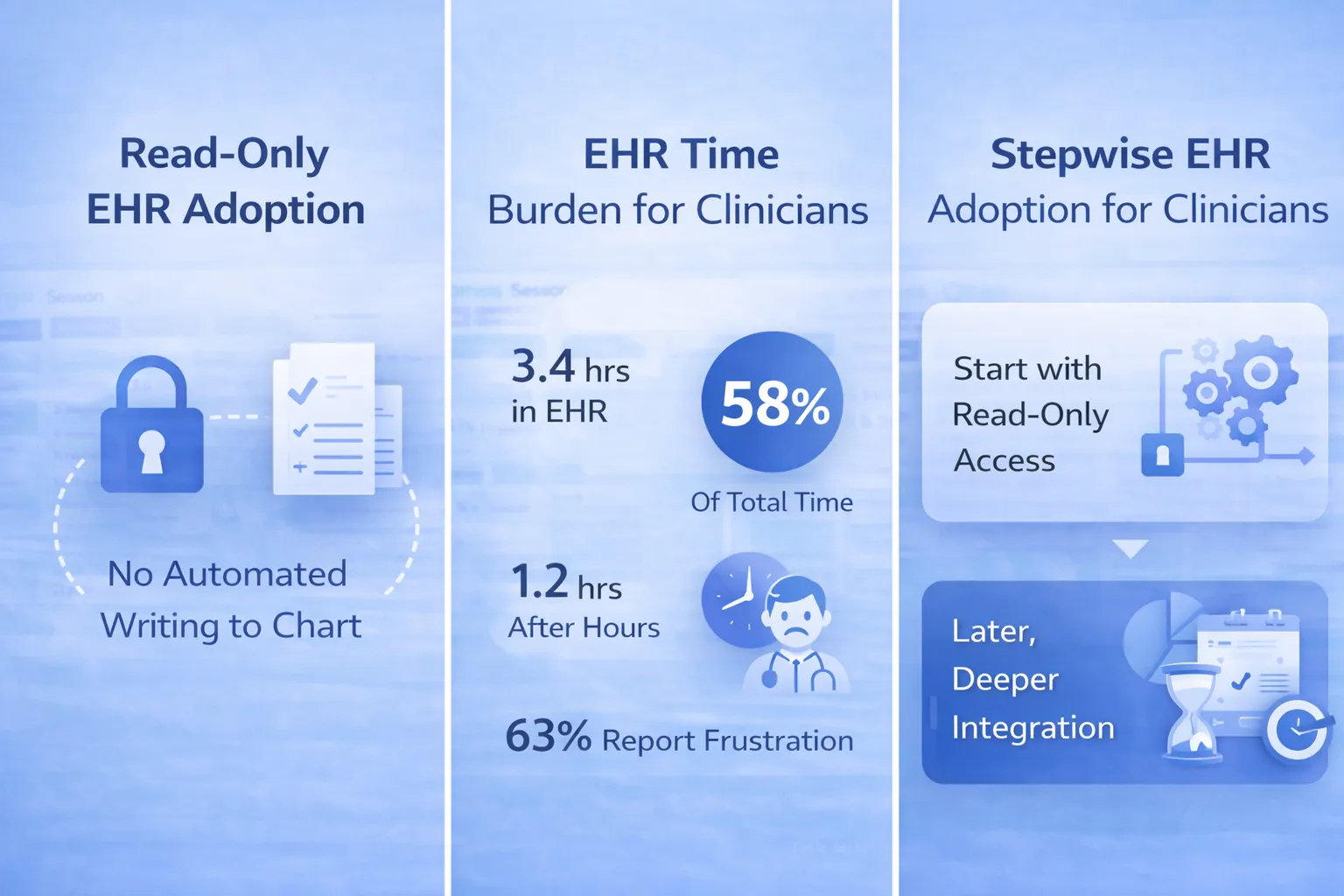
According to research cited by the American Medical Association, physicians spend an average of 3.4 hours of every eight scheduled clinic hours in the EHR, accounting for nearly 58% of their total time during patient-facing days. On top of that, clinicians spend another 1.2 hours after scheduled clinic time completing EHR work, plus additional time on unscheduled days.
The concern isn’t just technical, but also cognitive. Research shows the gap between the potential and actual benefits of EHRs is largely driven by cognitive burden and poor usability, which negatively impact clinical efficiency and data quality. In a survey of more than 4,000 physicians, 63% reported that EHRs added to their daily practice-related frustrations, and worse usability scores were linked to higher odds of burnout.
Against this reality, adding complex integrations, no matter how promising, can feel like more of a burden, not less.
What “Read-Only” EHR Adoption Really Means
Read-only EHR adoption does not write data directly into the EHR, but it securely reads existing clinical information, such as prior notes, medication lists, problem summaries, or uploaded PDFs, to gain context.
The AI then supports documentation outside the EHR: generating structured notes, medical record summarization, insurance documentation, referrals, or patient handouts. Clinicians can review, edit, and verify everything before manually copying or uploading content into the chart using their normal workflow.
Nothing is written automatically. Nothing changes in the EHR unless the clinician chooses. This model of medical software prioritizes clinician control while delivering meaningful administrative support.
Why Read-Only Is Often the Smarter First Step
- Faster implementation
Because read-only access avoids complex write permissions and interface development, onboarding can happen in days or weeks rather than months. For instance, a clinic could begin using a read-only AI scribe within a few weeks, gaining immediate relief without disrupting existing workflows. - Lower operational and compliance risk
Without automated chart updates, practices reduce the risk of incorrect entries and maintain clear clinician accountability. This approach also aligns with HIPAA requirements for data integrity. - Higher clinician trust
Clinicians are more likely to adopt AI when they remain in full control of the medical record. Verification-first workflows feel supportive, not intrusive. - Immediate value without workflow disruption
Read-only systems fit into existing documentation habits, minimizing training time and resistance from staff. This represents seamless AI adoption, a technology that adapts to clinical practice, not the other way around.
Where Documentation-First AI Fits In
Documentation-first AI platforms are designed to support, not replace, clinical workflows. They focus on capturing clinician-patient conversations, structuring documentation like SOAP notes, summarizing long medical histories, and generating administrative outputs, such as referrals and patient handouts with traceable source references.
When paired with read-only EHR access, these systems gain the context they need to be useful, without crossing into automated charting or medical decision-making. This balance is especially important for practices prioritizing accuracy, compliance, and clinician oversight.
For instance, if a dentist wants to review a patient's 40-page surgical history before a complex extraction, the AI medical Scribe (lightweight medical software solution) with read-only access can summarize medical conditions and current medications in minutes, while the dentist verifies accuracy and makes the final determination.
Building Toward Sustainable AI Adoption
Read-only EHR adoption isn’t a limitation, but it’s a foundation. Clinicians can experience the benefits of read-only EHR-integrated AI documentation, build confidence in accuracy and workflow fit, and decide later whether deeper integration is needed.
By starting small and staying clinician-led, practices avoid unnecessary disruption while still moving forward. In healthcare, sustainable AI adoption isn’t just about speed, but it’s also about trust.



